
Two-layer technique after anterior tooth trauma
Many different techniques have been proposed for the restoration of traumatized or aesthetically compromised anterior teeth. Most of them require the use of multi-layering procedures which most of the times are extremely complicated for the general practitioner.
Nowadays it is possible to use a simplified approach with a material which only requires a two layering procedure (dentin and enamel), as it was the case with this young patient.
The patient, Y. 9 years old, showed up at our dental office after a trauma involving the frontal area of his mouth.
Once it was determined that it was a simple accident (the boy had been playing with some friends when he fell), he was examined.
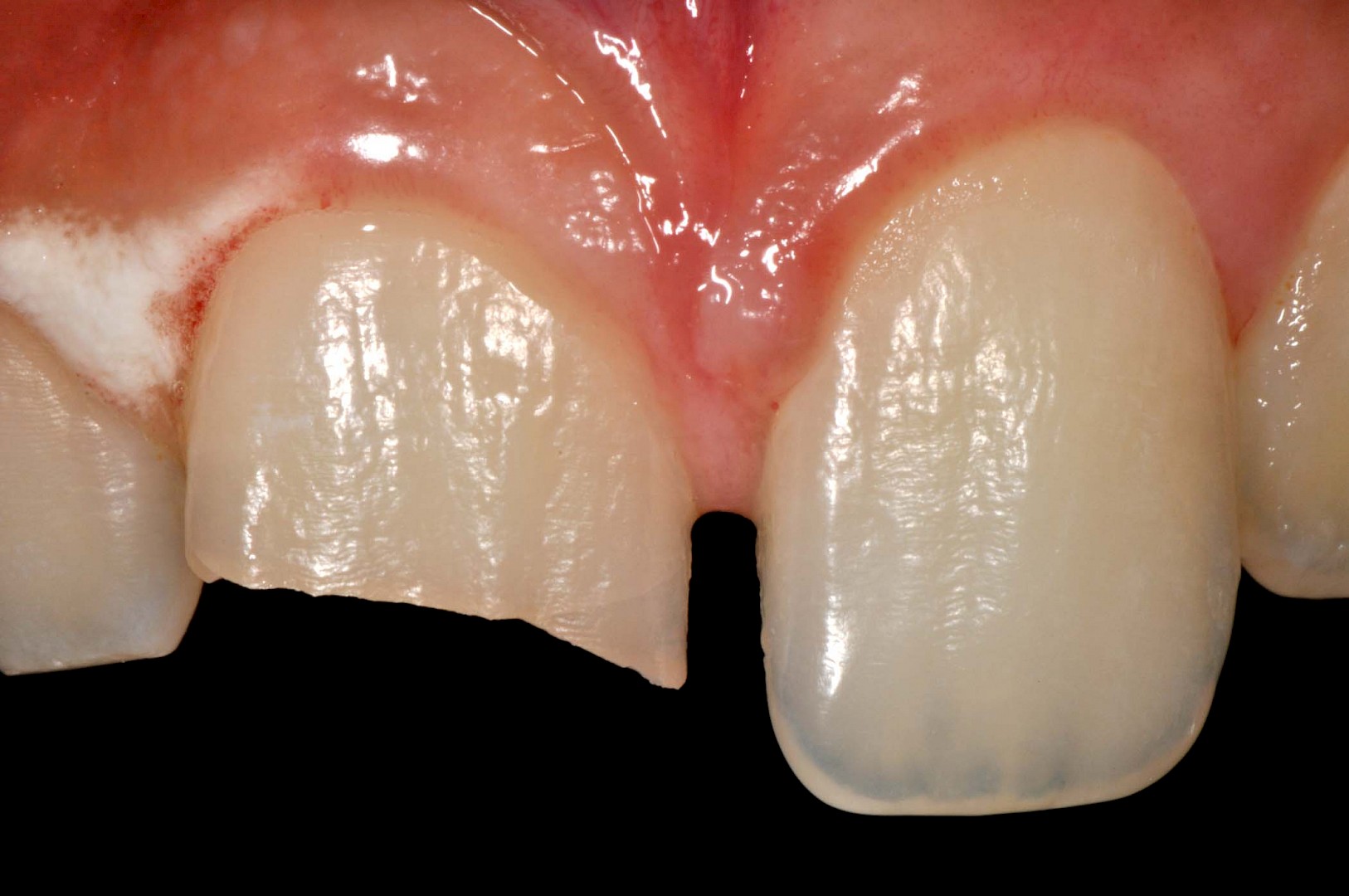
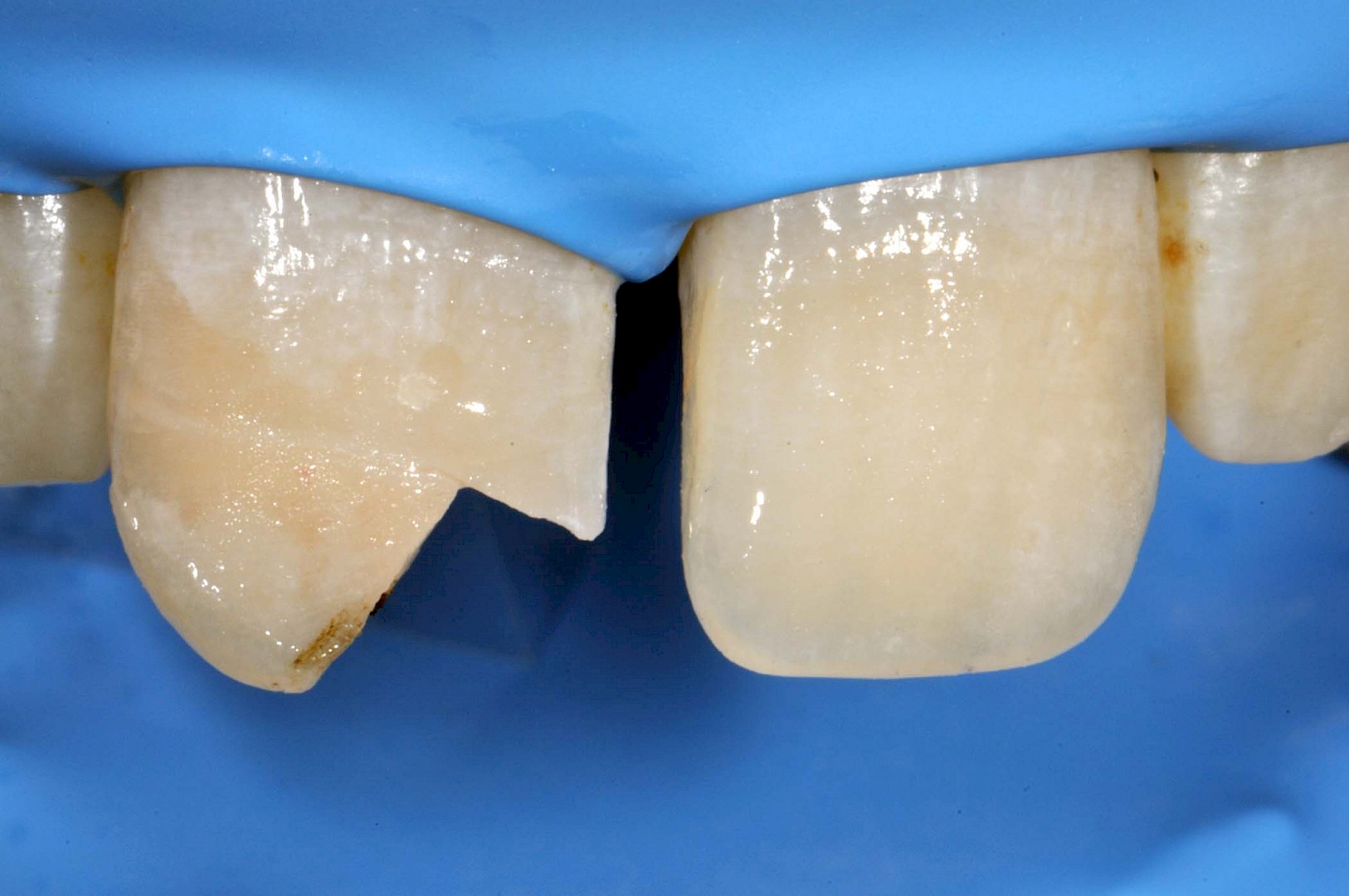
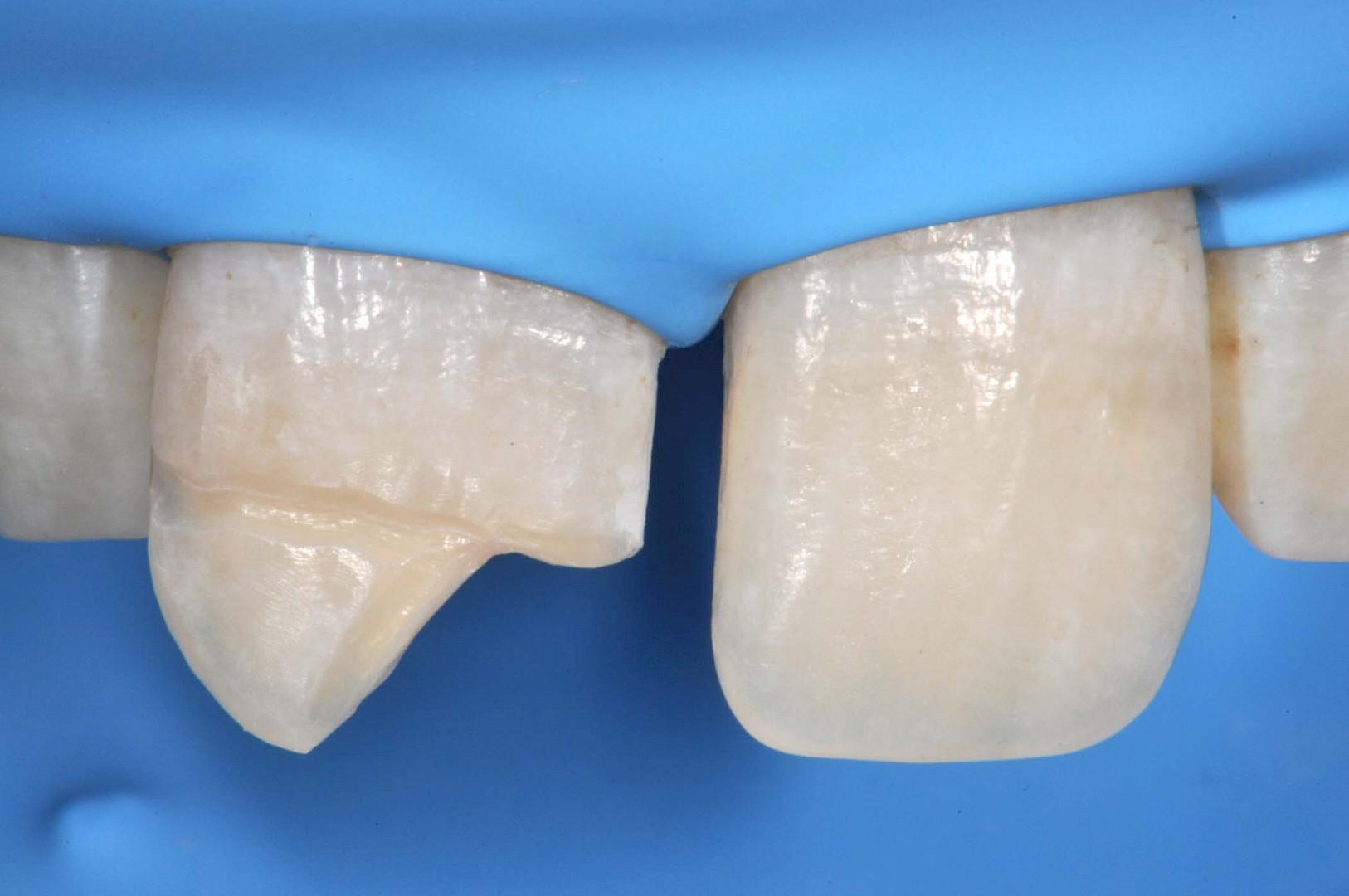
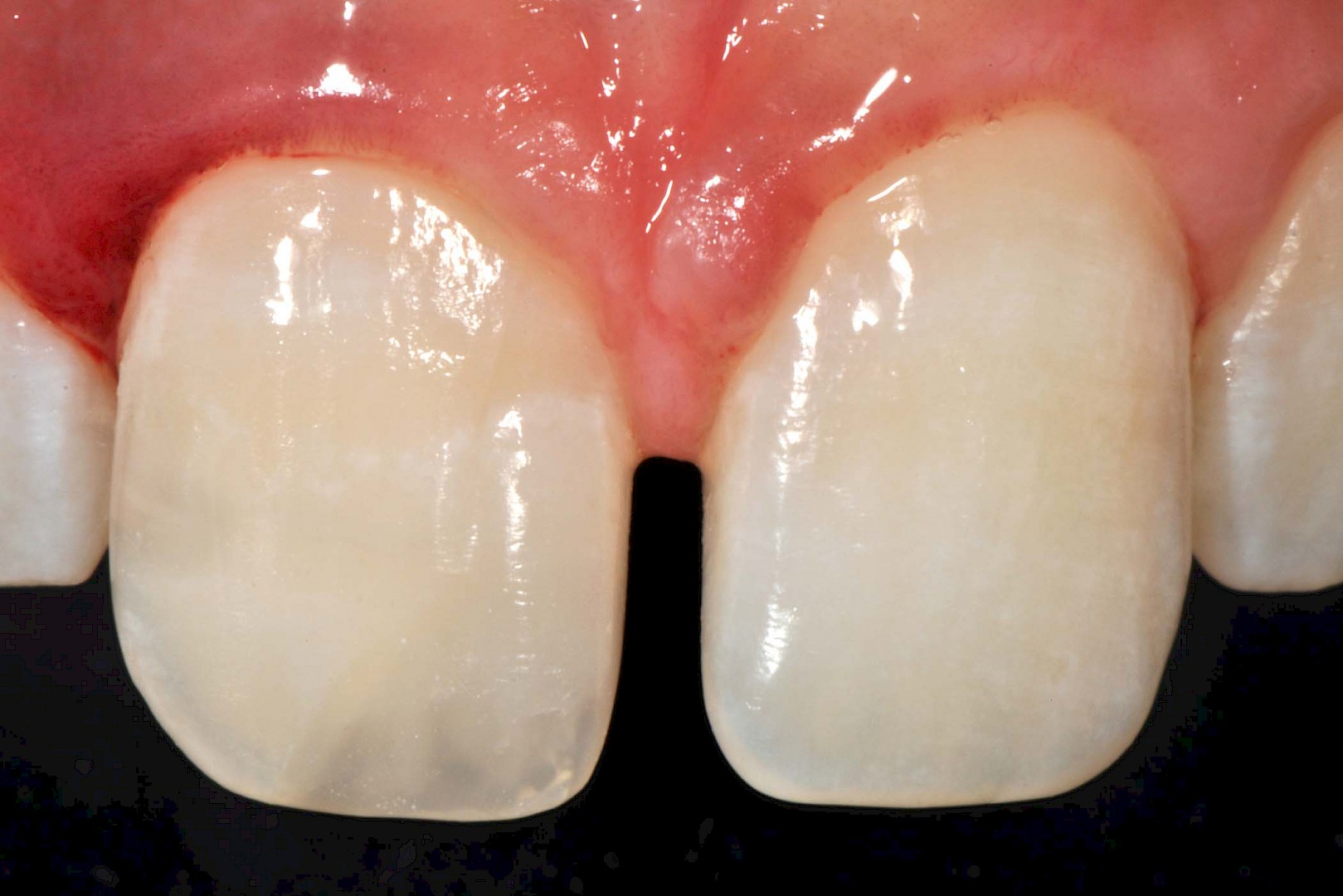
On examination the patient was found to have a fracture (Ellis class III with pulpal exposure) on tooth 1.1, physiological mobility of the tooth itself and of other teeth, a slight swelling on the inside of his upper lip, slight pain and poor plaque control.
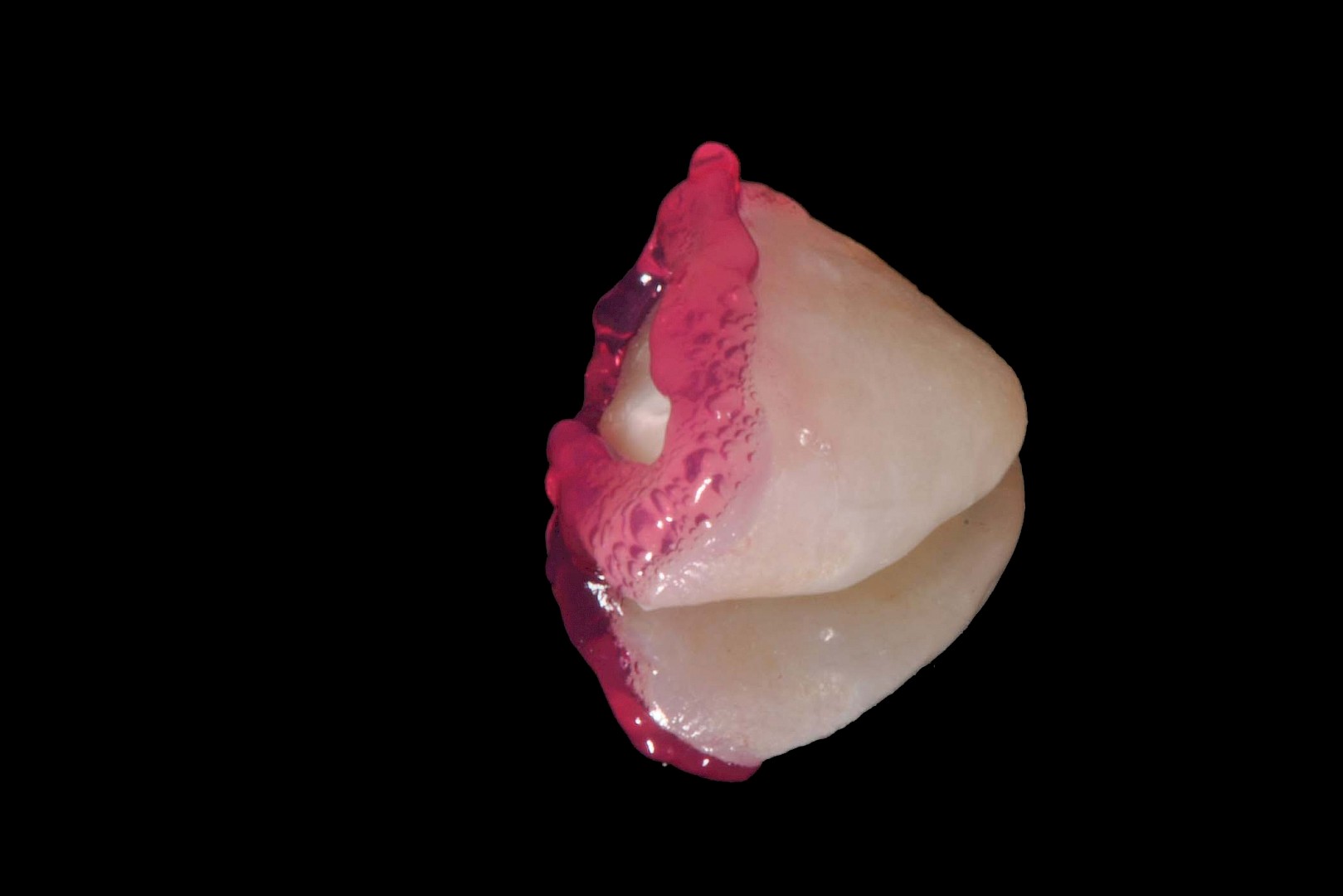
The patient had the fractured fragment with him, which was immediately immersed in physiological solution.
The pulpal exposure was small and not bleeding, so the decision was taken to proceed with the reattachment of the fragment and the direct reconstruction of the missing portion.
After a local anesthesia with articaine, the operative field was prepared. Placing the rubber dam was quite difficult due to the mixed dentition of the patient.
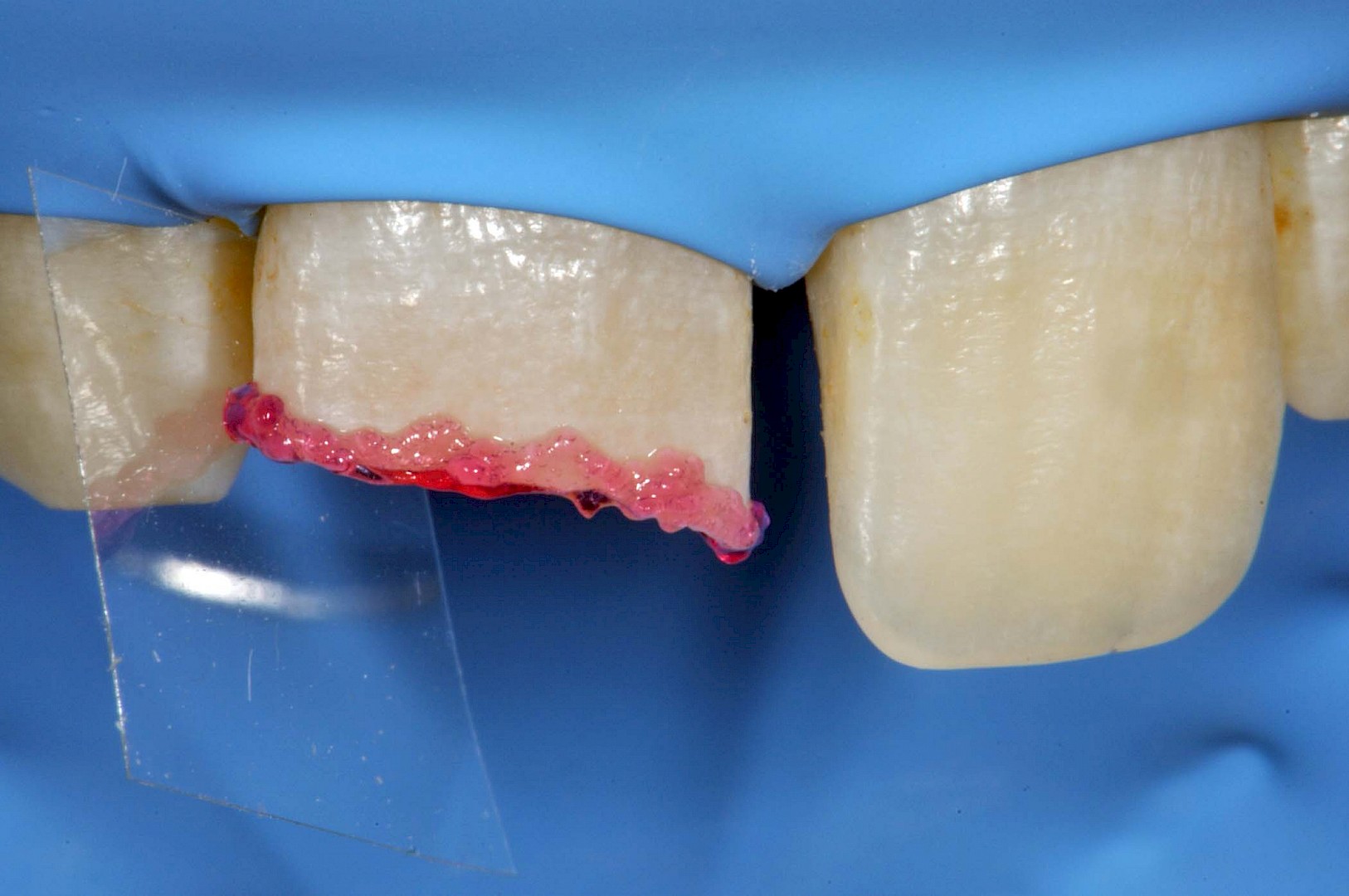
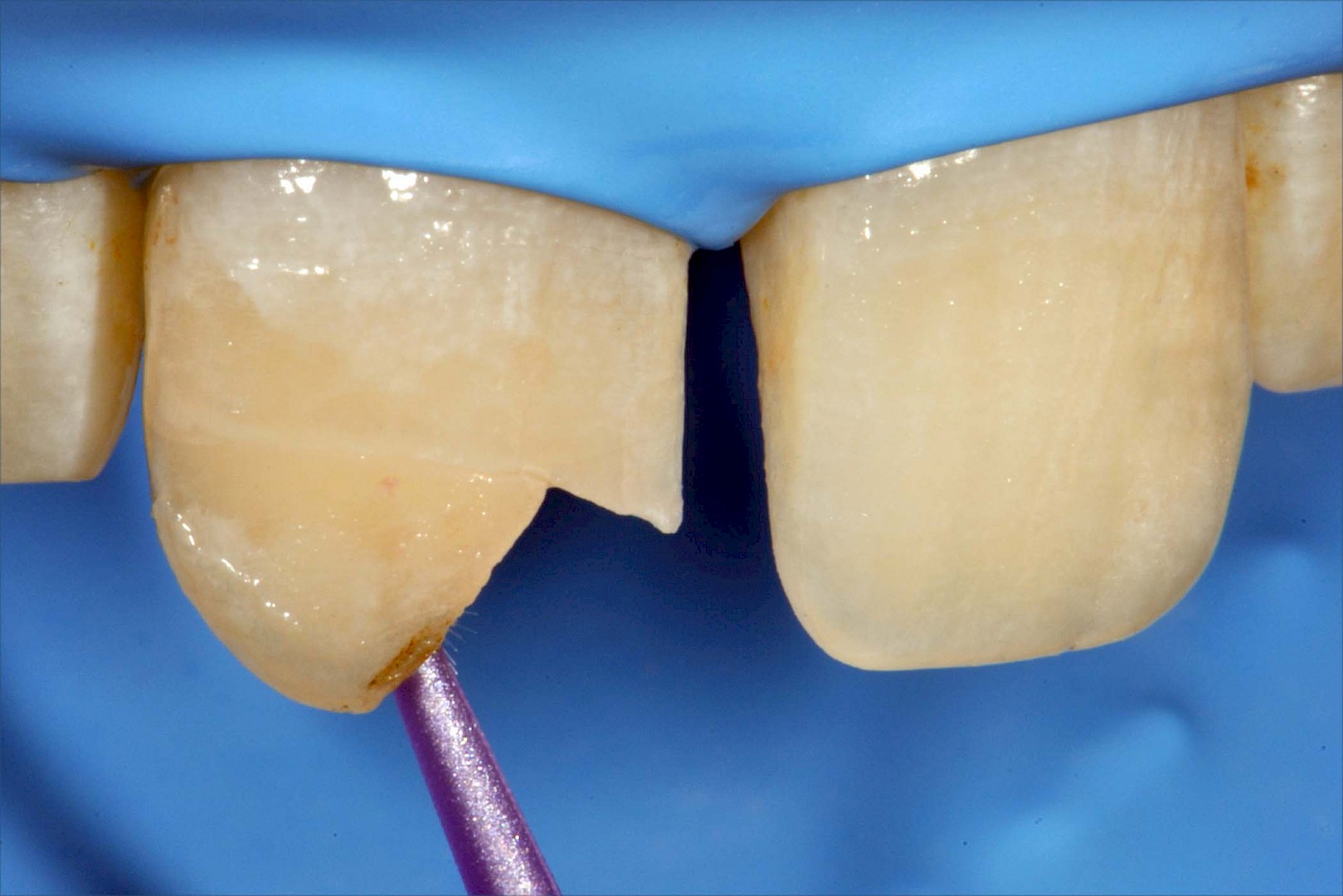
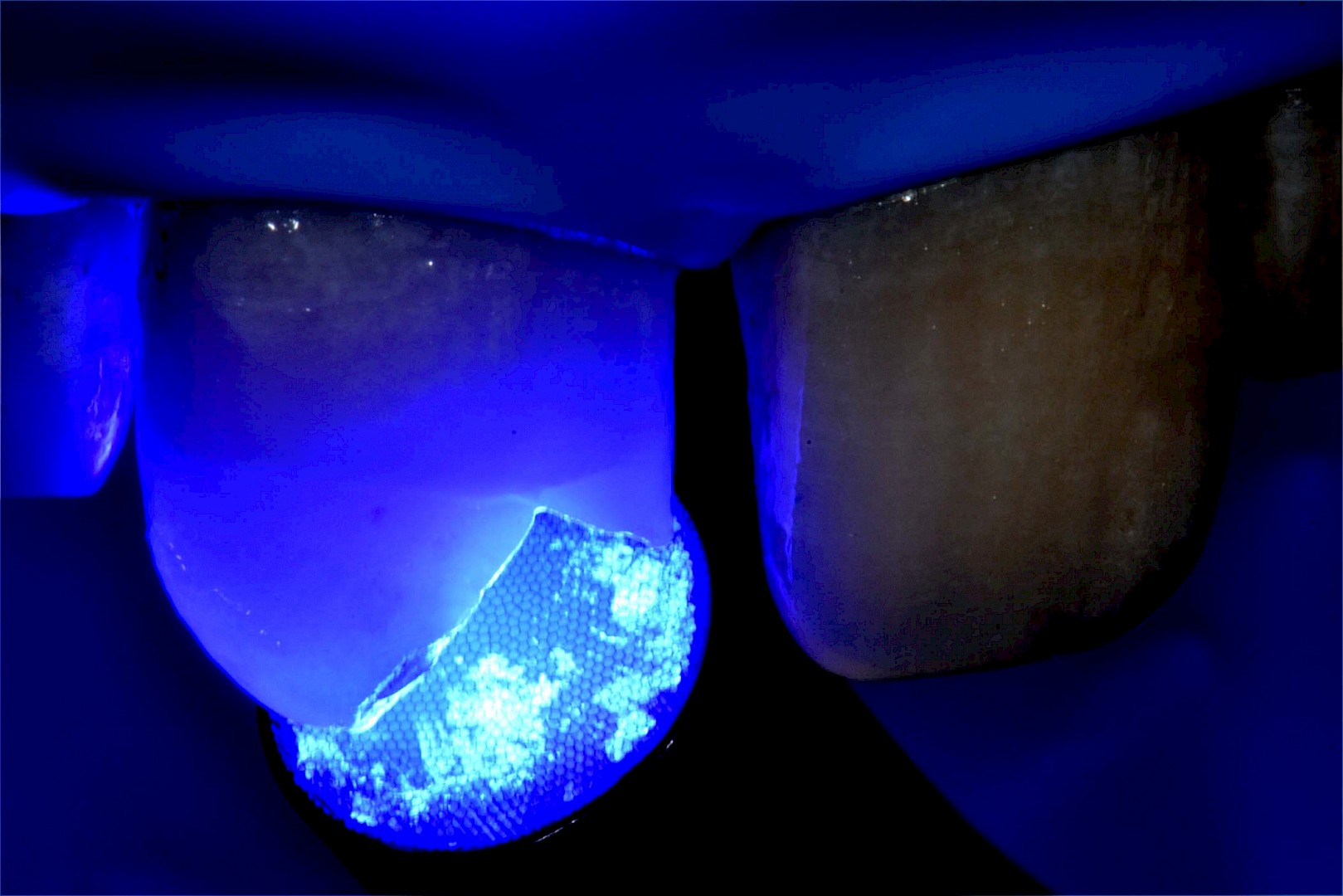
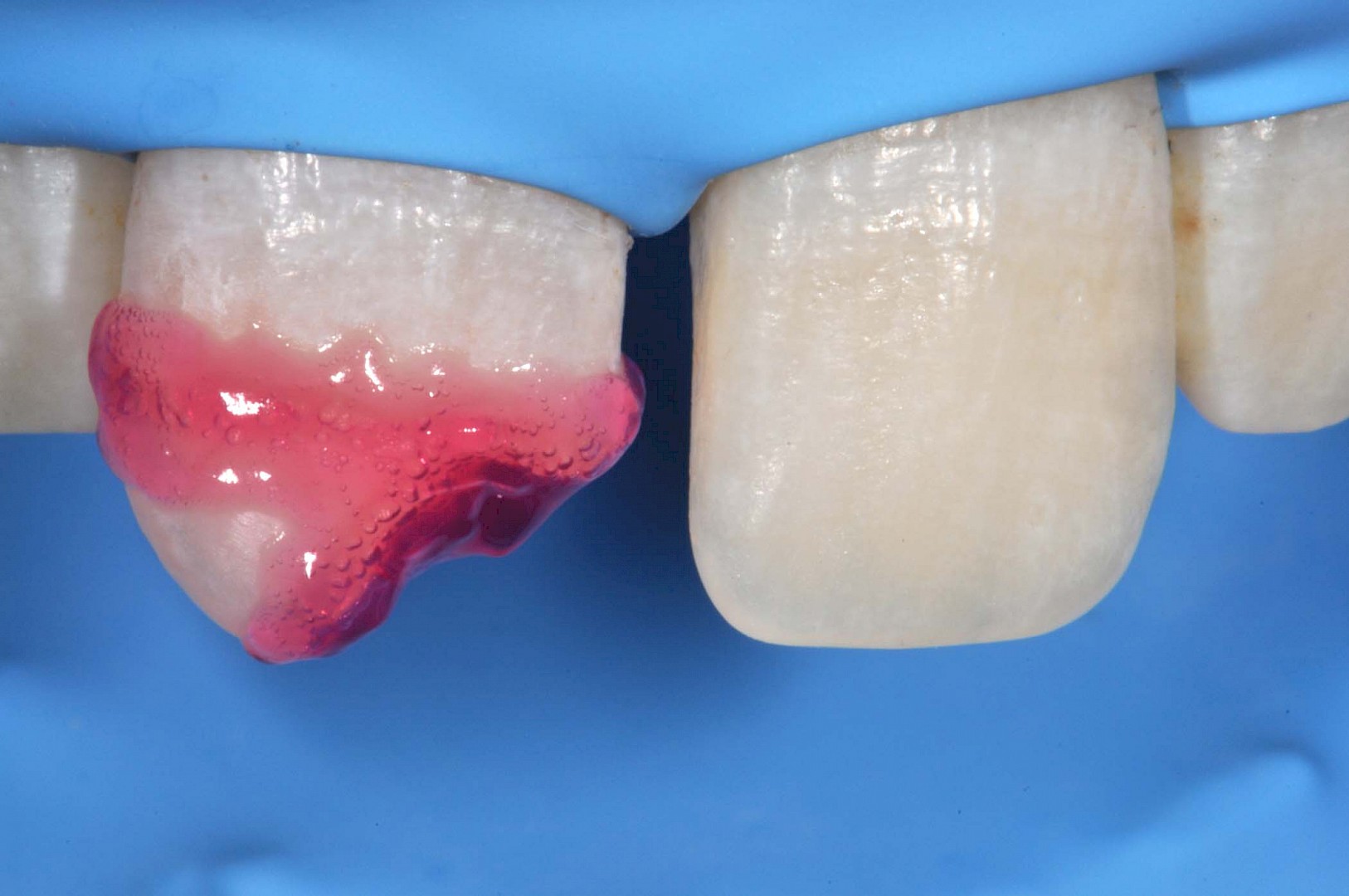
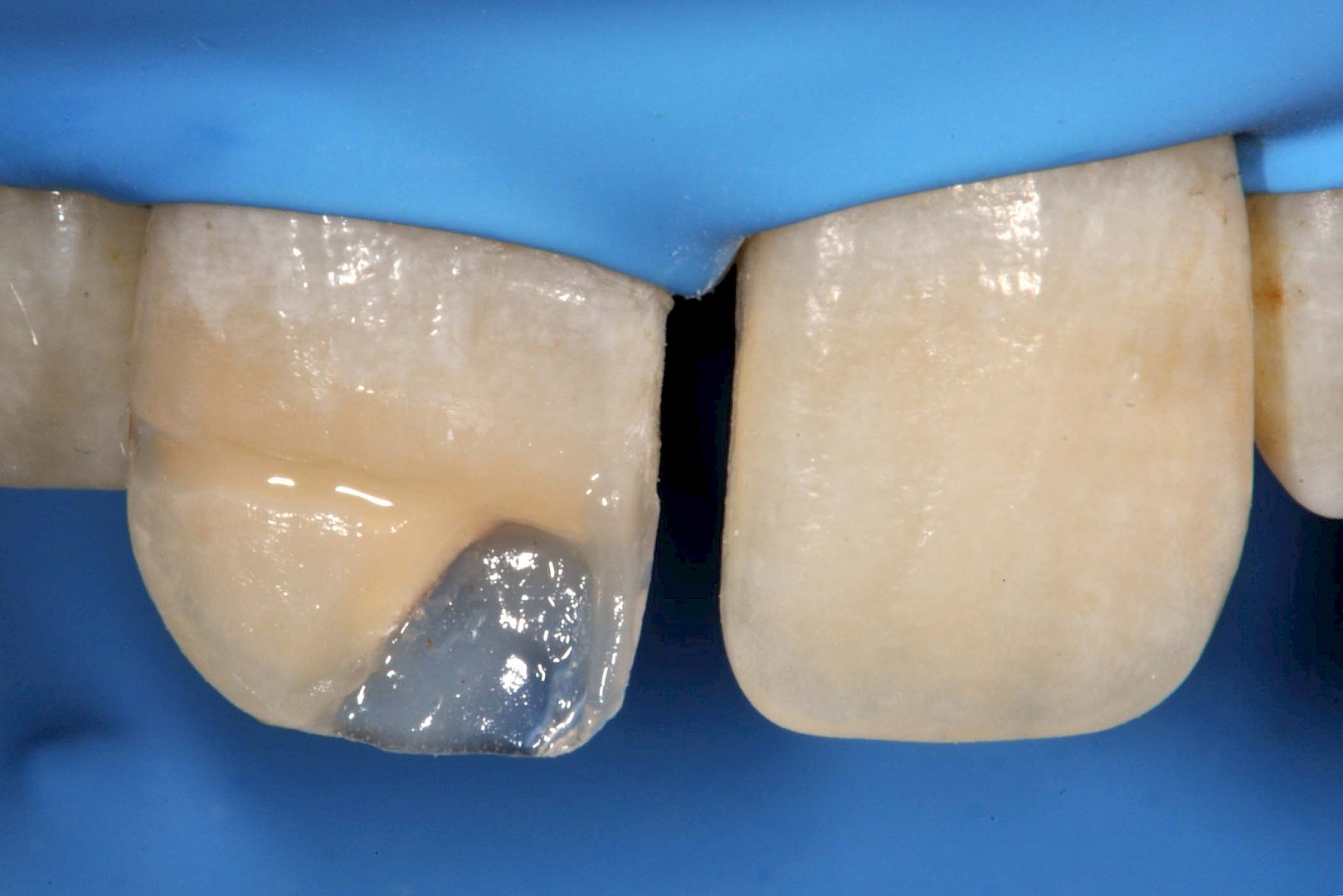
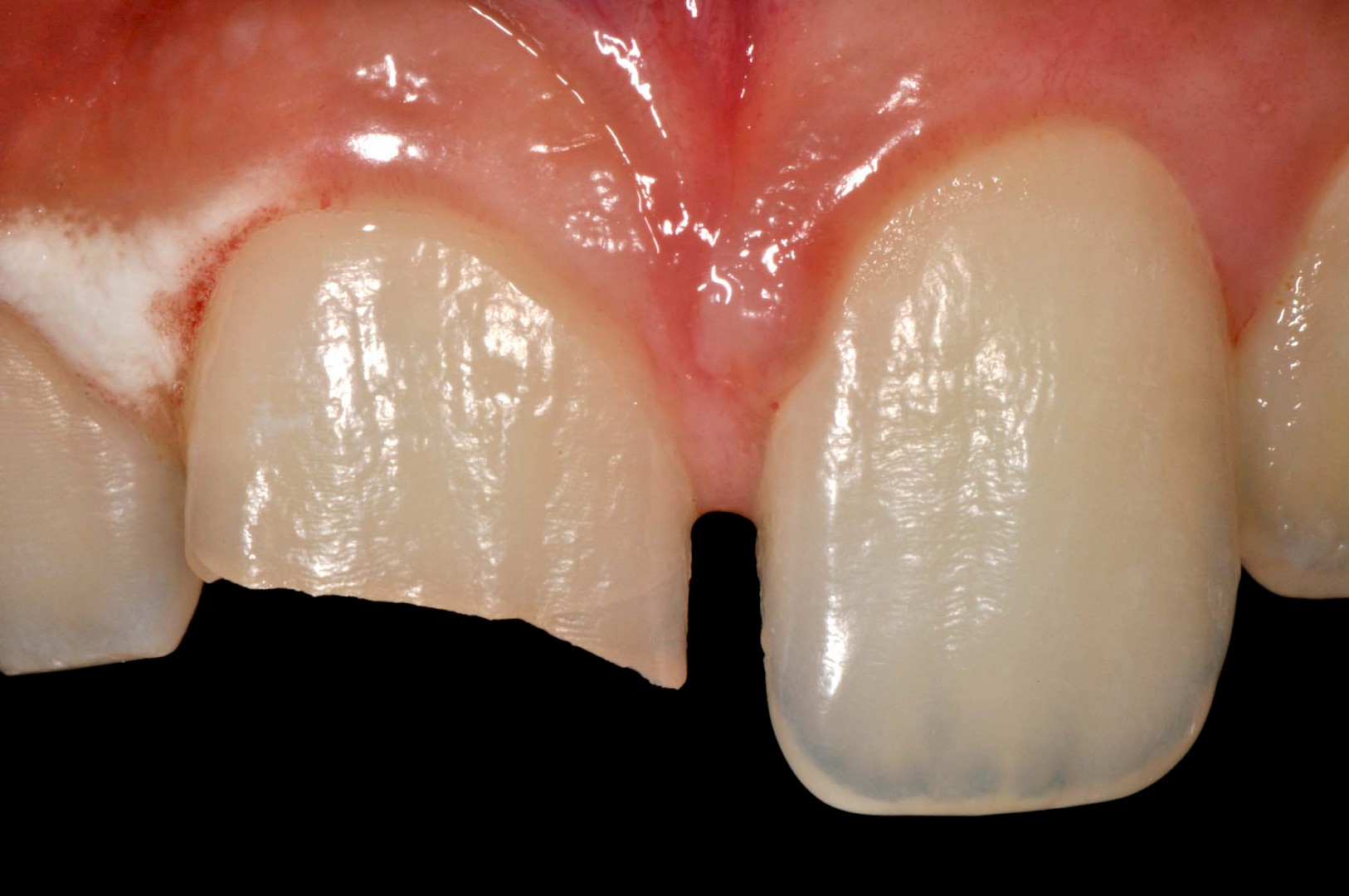
The surface area was lightly cleaned using a toothbrush, after which the adhesive system EE-BOND & ETCHING-GEL HV by Tokuyama Dental (7 ^ generation with enamel etching) was applied both on the tooth and on the fragment. The latter was repositioned with interposition of a thin layer of flowable composite.
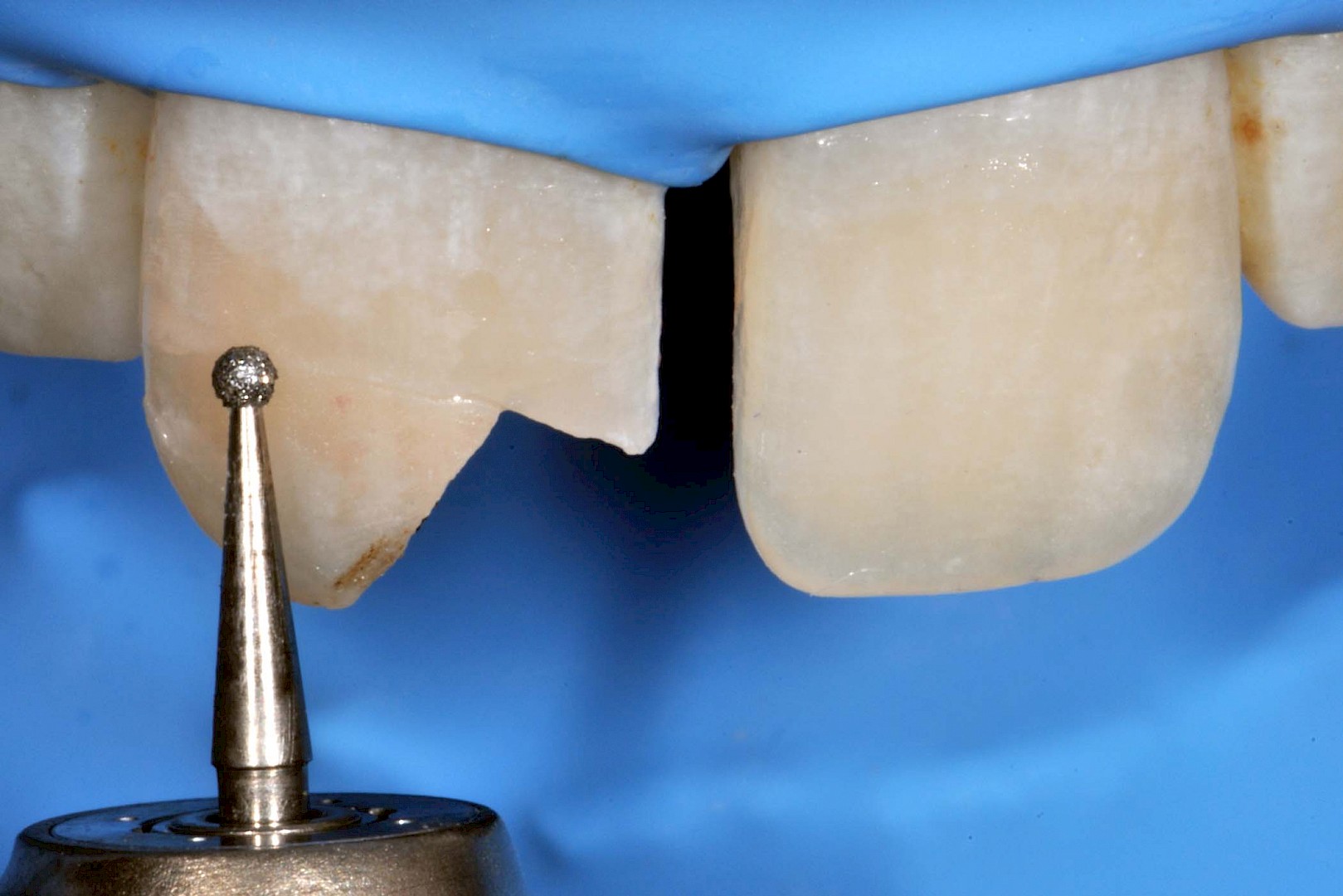
After curing, a double bevel was created along the fracture line, both on the vestibular and the palatal sides. This was performed to increase the adhesive strength of the fragment, to give it regular margins, and to allow the direct restoration of the missing part.
The adhesive system was applied once again, and a freehand stratification was carried out.
The initial aesthetic analysis had shown the presence of a marked area of incisal translucency and a clear halo on the edge.
NE (ESTELITE ASTERIA by Tokuyama Dental) was applied as a first layer on the palatal side, followed by a buildup of body A2. Following the manufacturer’s instruction, the body was applied as far as the medium third surface, while room was left for a thin layer of enamel NE in the incisal third.
To recreate the enamel translucency, TE was used between the body mamelons, while the halo was reproduced using body A2.
After finishing and polishing, the patient was sent home and contacted periodically in the following days for news on possible pulpal symptomatology.
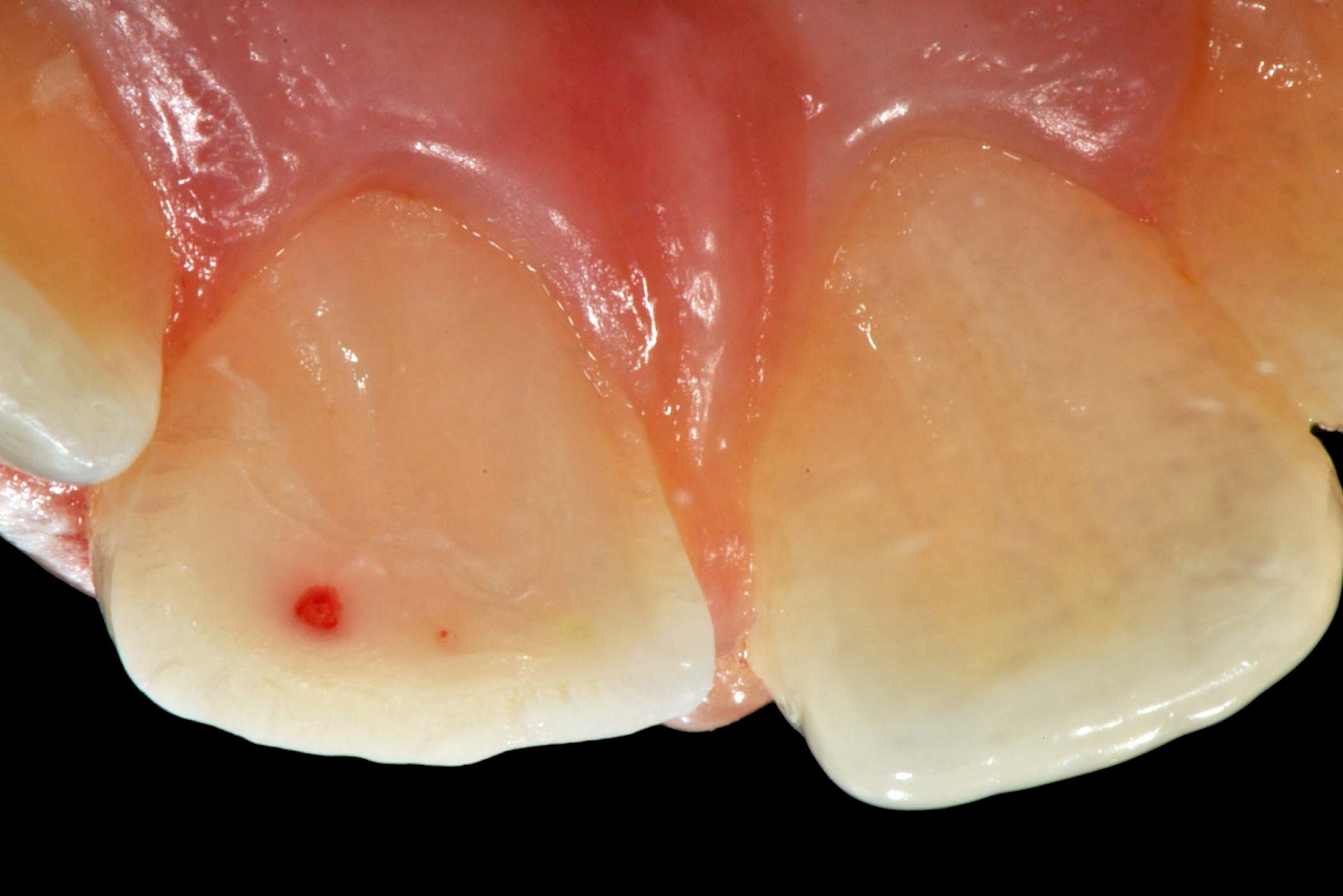
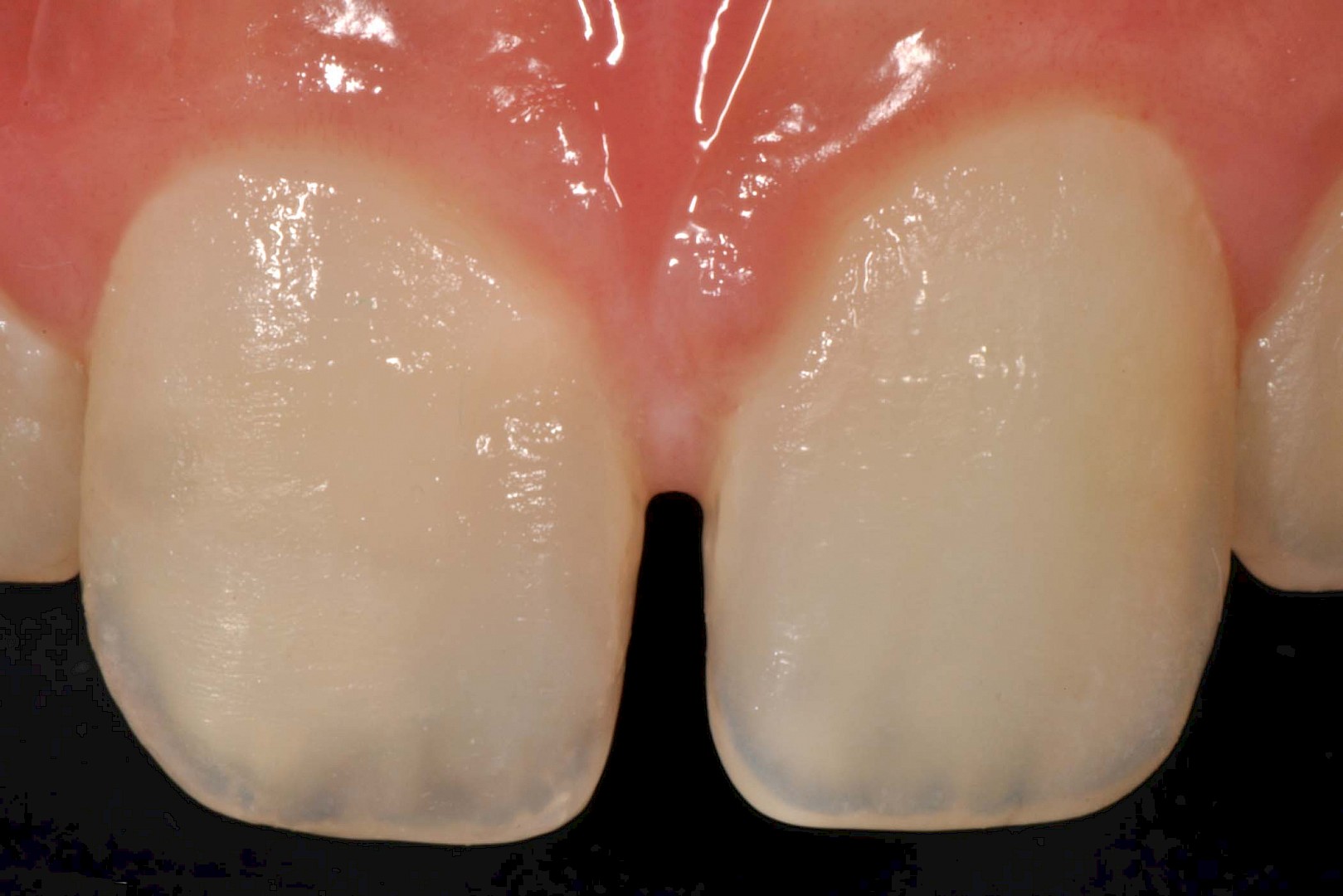
In the control picture at 7 days, the excellent integration of the restoration can be appreciated. The integration of the composite used, and the simplicity of the layering procedure, have enabled us to immediately achieve a satisfactory result without need of re-treatment.



Conclusion
The body shade has splendidly masked the line of transition between the tooth and the restoration, while the enamel NE and the translucent TE have created an incisal area which looks completely natural.
The patient was satisfied with the aesthetic appearance of the restoration, and in the final picture a one week post-op control after the rehydration of the adjacent teeth is shown.

Author:
Prof. Dr Simone Grandini D.D.S, MSc, PhD
Chair and Professor of Endodontics and Restorative Dentistry, University of Siena, Italy
Head of Department of Endodontics and Restorative dentistry, University of Siena, Italy
Dean of the School of Dental Hygienists
https://www.styleitaliano.org/author/simone-grandini/

Author:
Dr Giulio Pavolucci
Visiting Professor in Restorative Dentistry and Endodontics, in the University of Siena, Italy
Employment in private dental practice (Cortona, Italy) with focus on on restorative dentistry and endodontics
Active member of the Italian Society of Restorative Dentistry (SIDOC)
https://www.styleitaliano.org/author/giulio-pavolucci/