

Simple, quick and aesthetically pleasing
When I was introduced to Tokuyama’s shadeless OMNICHROMA composite by Gillien Duncan, my local Trycare representative, I was curious to see if it could work. I didn’t believe the claims that one completely shadeless material could mimic all the myriad of shades found in teeth.
However, I was keen to see how it would handle in my hands and wondered if it would be a good enough material to use in my practice. So, I decided to buy a pack and find out. I decided to have a go on an extracted tooth and the results persuaded me to go ‘live’ on my first patient. In the following series of case studies, you will see the results of my first four cases.
Case 1
This was a 24-year-old female patient requiring small incisal build-ups on teeth UL1 and UL2. There was nothing of note in the medical history and the periapical radiograph showed good bone, some existing intact restorations and no evidence of caries. Before photographs were taken, using polarised photography in order to remove the surface reflection and aid proper shade evaluation. ESTELITE SIGMA QUICK shade OA2, ESTELITE SIGMA QUICK A2 and OMNICHROMA were compared to evaluate which shade would match best. The OMNICHROMA was selected. Because it was a minimal restoration, in enamel only, no local anaesthetic was required. The margins were bevelled with a red flame diamond high speed bur. The enamel was then acid-etched and TOKUYAMA BOND FORCE II applied.
TOKUYAMA BOND FORCE II is a one bottle adhesive that only requires one single application. It can be used on both cut and uncut enamel and dentine. You can choose to use it using either a self-etch or selective enameletch technique. I prefer to use the selective enamel-etch technique. It gives an extended five minutes working time and only requires 10 seconds to light-cure.
The OMNICHROMA restoration was then built up freehand, no palatal stent was required on this occasion, and then the OMNICHROMA was light-cured for 20 seconds. Immediately upon light-curing the previously opaque material transformed into a translucent restoration, which seamlessly merged with the surrounding teeth and disappeared like magic. The occlusion was checked, smoothed and then a final high lustre polish created using a Dentsply Enhance polishing disc then Cosmedent flexi mini disc kit. The patient was shown the final restoration and departed extremely happy with the final result.
















Case 2
This was a 23-year-old male patient who had lost a distal restoration from his upper right central incisor and needed a quick replacement with very little time available. The tooth was caries-free and consequently no local anaesthesia was required. The margins of the restoration were bevelled using the high-speed turbine and a red flame diamond bur.
Polarised photography was used to check the value or brightness of the material. The enamel was then acidetched and TOKUYAMA BOND FORCE II applied.
The OMNICHROMA restoration was then built up freehand using OMNICHROMA BLOCKER on the palatal surface, this was light-cured for 20 seconds and then the labial surface built up using regular OMNICHROMA. An oxygen inhibition gel was applied and then the OMNICHROMA was light-cured for 20 seconds. The occlusion was checked, the excess removed, the restoration smoothed and then polished to a final high lustre polish using the high-speed turbine and slow speed handpiece.
The patient was shown the final result and was delighted.




Case 3
This was a 27-year-old female patient with an unsightly mesial incisal composite on her upper left central incisor with associated wear. There was nothing of note in the medical history. Articaine local anaesthetic was administered and the occlusion checked.
The deficient restoration was removed using the high-speed turbine leaving a caries-free preparation. The enamel was then acid-etched and TOKUYAMA BOND FORCE II applied. The restoration was then built up freehand using OMNICHROMA and OMNICHROMA BLOCKER. The occlusion was checked and then the restoration smoothed and polished. The patient left the practice very happy.


Case 4
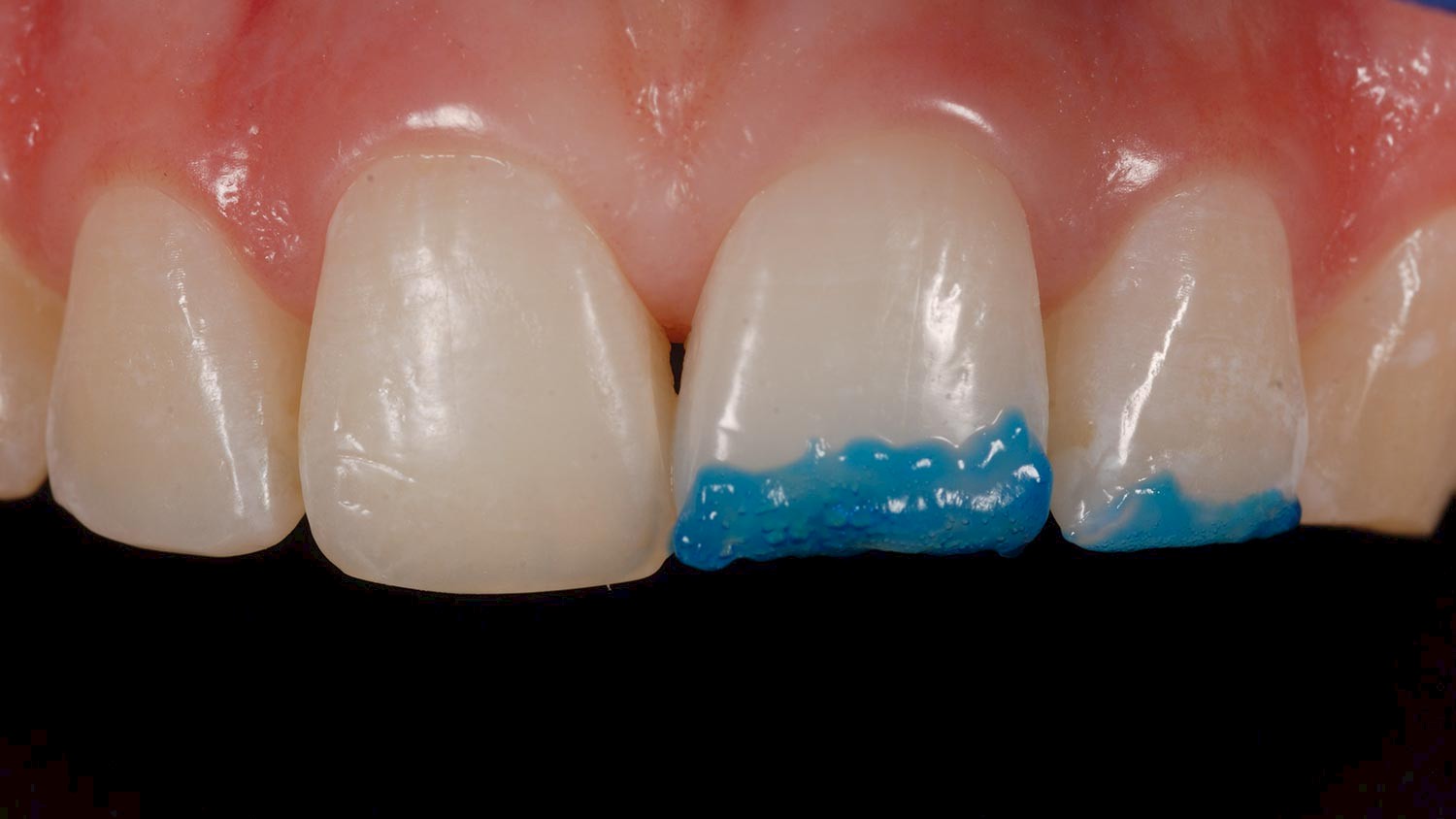
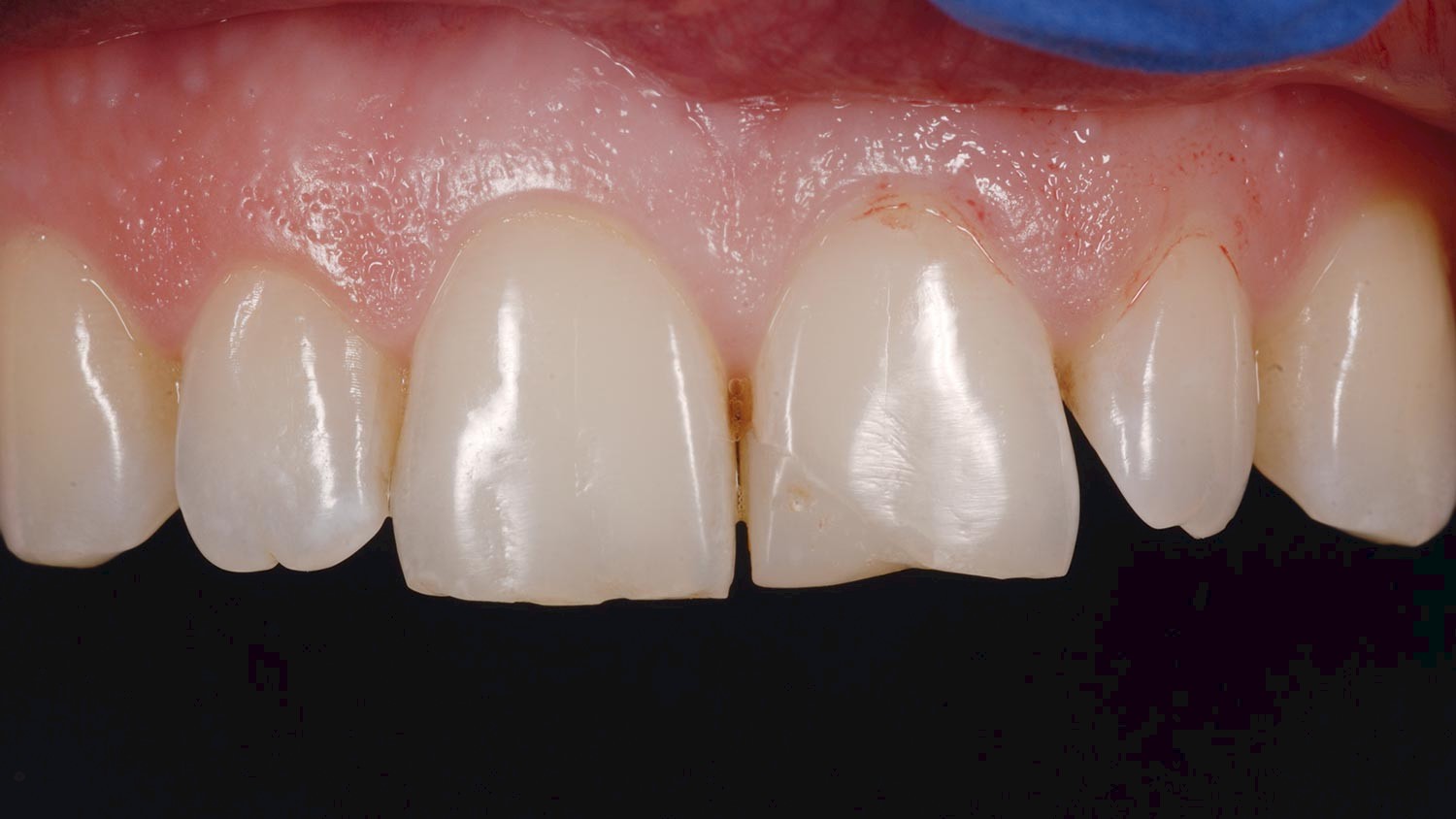
This was a 65-year-old female patient with a fractured mesial incisal composite on her upper right lateral incisor. The patient was complaining of a ‘broken front filling’. The medical history was updated. On examination, the mesial incisal restoration on the upper right lateral incisor was broken and required replacement. The patient was happy to proceed there and then.
A lignocaine 1:80000 infiltration local anaesthetic was administered and the occlusion checked. The deficient restoration was removed using the high-speed turbine and the margins of the preparation bevelled. The preparation was caries-free. The enamel was then acid-etched and TOKUYAMA BOND FORCE II applied. The restoration was then built up freehand using OMNICHROMA and ESTELITE SIGMA QUICK shade OA3. The occlusion was checked and then the restoration smoothed and polished. The patient was shown the final result and was delighted.




Conclusion
Since starting with OMNICHROMA I have been very impressed with the results. In particular, I enjoy the handling characteristics, the surface polishability and the way that it seamlessly blends in with the surrounding teeth to provide a very harmonious restoration without the complexity of layering techniques. OMNICHROMA comes in two varieties: regular, which has a natural translucency built into it, which only becomes apparent when it is light cured, and an opaque OMNICHROMA BLOCKER, which is designed to mask over dark stains or for use on incisal edges etc, where you do not want the dark shadow of the mouth to affect to otherwise superb aesthetic result of OMNICHROMA. In my experience, I use the OMNICHROMA BLOCKER in about one in four restorations.I’ve been delighted with the aesthetic results I can achieve with OMNICHROMA and it definitely has a role to play in my practice, particularly when I am matching a tooth that does not have a complicated colour range and structure that would require a layering technique. In a large number of cases, OMNICHROMA can provide a highly aesthetic result.

Author:
Dr Peter Buchan
Clinical Director of No9 Dental Practice
Award-winning Cosmetic Dentist
Accredited by the BACD in Cosmetic Dentistry
Diploma in Implant Dentistry from the Royal College of Surgeons Edinburgh
Winner of the Aesthetic Dentistry Award 2018
No9 Dental Practice Ltd
29 West Main Street
Uphall
West Lothian
EH52 5DN